Best Practices in the Area of Seating and Mobility—A Study Utilizing the Delphi Technique
Mary Isaacson
ABSTRACT
The Delphi technique was used to gather data from a group of experts regarding their perceptions of best practices in the area of seating and mobility. The data was analyzed to answer the question “so what?” As a result of the data elicited from this panel of expert practitioners in the area of seating and mobility, best practices can be defined as a multi-variant complex series of interactions in which the clinician uses experience, hands on techniques, skills, technology, resources, self-directed learning, follow-up, and a relationship with the consumer in the provision of services.
KEYWORDS
Best Practices, seating and mobility, Delphi technique
INTRODUCTION
“Best practices are a professional’s decisions and actions based on knowledge and evidence that reflect the most current and innovative ideas available” (1) The purpose of this study was to describe perceptions of occupational and physical therapists who specialize in seating and mobility evaluations about current best practices in the field. This was accomplished by using a Delphi technique to gather data from the leaders in the field regarding their perceptions of best practices in the area of seating and mobility.
The following research questions were addressed in the study:
- What skills are needed to adequately perform wheelchair assessments?
- What do occupational and physical therapists who are practicing in the filed of assistive technology consider to be best practices?
- How are these skills for best practices acquired and how are they maintained?
METHODS
A descriptive research design, the Delphi technique, was utilized in this study. The Delphi technique facilitates effective interaction between a panel of geographically dispersed experts (2). Researchers utilize the Delphi technique to translate professional experience and knowledge into informed judgment, resulting in advanced clinical decision making (3). The Delphi technique has a number of strengths and limitations (Table 1).
| Strengths | Limitations |
|---|---|
| Study of a geographically dispersed respondents who are considered experts in the field of study. | Expert “opinion” may be considered qualitative in nature. Expert must clearly be defined. |
| Anonymity of the group limits peer persuasion | Annonymity may be considered to lead to a lack of responsibility. |
| Discussion of broad complex problems | Delphi results may represent a “moment in time” for the respondents. |
| Time and cost effective | Quality of the Delphi rests on the quality of the design. |
| Note: Adapted from: (10). | |
The expert practitioner had to be well defined and then identified for this study. Subject selection criteria on expertise have been developed to identify potential experts (4). Expert criteria includes: having seven or more years of clinical practice, being involved in direct patient care at least 50% of the time, having completed formal or informal advanced work in the specialty area, and being someone to whom the nominator would refer a patient with complications or a family member for care. These criteria served as the baseline criteria for this study.
| Profession | Residence | Years in profession |
|---|---|---|
PT |
Florida |
33.5 |
OTR |
Illinois |
24 |
PT |
Massachusetts |
23 |
OTR |
Louisiana |
23 |
PT |
North Carolina |
21 |
PT |
New York |
19 |
PT |
Atlanta |
19 |
PT |
Oklahoma |
18 |
OTR |
Colorado |
18 |
PT |
Pennsylvania |
17 |
OTR |
Pennsylvania |
14 |
PT |
Colorado |
14 |
PT |
Pennsylvania |
13 |
OTR |
New York |
10 |
PT |
Washington |
10 |
A total of 15 experts comprised the sample for this study (Table 2). The expert panel exceeded the defined criteria for an expert. Experience of the panel ranged from 10 through 33.5 years with the average 18.4 years. One-third of the participants were occupational therapists (OTR), and two-thirds of the participants were physical therapists (PT). The participants were geographically diverse and were from 12 states throughout the United States.
Qualitative data were collected through responses to the open-ended questions, and quantitative data were collected through responses to questions regarding demographic information. Quantitative data were transferred to SPSS for analysis, and qualitative data were transferred to a word processing program for analysis.
The qualitative data were then organized, tabled, and coded so that an objective, systematic and general description of the overall text was obtained.
RESULTS
Round One
In Round 1, the panel of expert practitioners answered questions thoroughly and completely. As a result, three overall themes emerged from the data. These themes were experience, knowledge, and sensitivity to the consumer’s needs. Throughout all of the answers, the need for experience consistently emerged. Sensitivity to consumer’s needs was also recognized as a necessity. This group of expert practitioners recognized that although they may have the experience, skills, and knowledge to complete the seating and mobility evaluation, it is irrelevant without input from the consumer.
Round Two
In Round 2, this group of expert practitioners elaborated, expanded, and confirmed results of the data from Round 1. Experience, knowledge, and the importance of consumer participation continued to be evident in this round. However, this round also resulted in a prioritization of specific skills and knowledge needed for completion of a thorough seating and mobility evaluation and specific strategies and details utilized by these practitioners to gain these skills and knowledge. These practitioners further expanded on barriers which exist in the area and seating and mobility, and strategies which they have utilized to overcome these barriers. As a result of data elicited from this panel of expert practitioners in the area of seating and mobility, best practices can be defined as a multi- variant complex series of interactions in which the expert clinician uses experience, hands on techniques, skills, technology, resources, self-directed learning, follow-up, and a relationship with the consumer in the provision of services.
DISCUSSION
 FIG. 1. The Wheel
FIG. 1. The Wheel
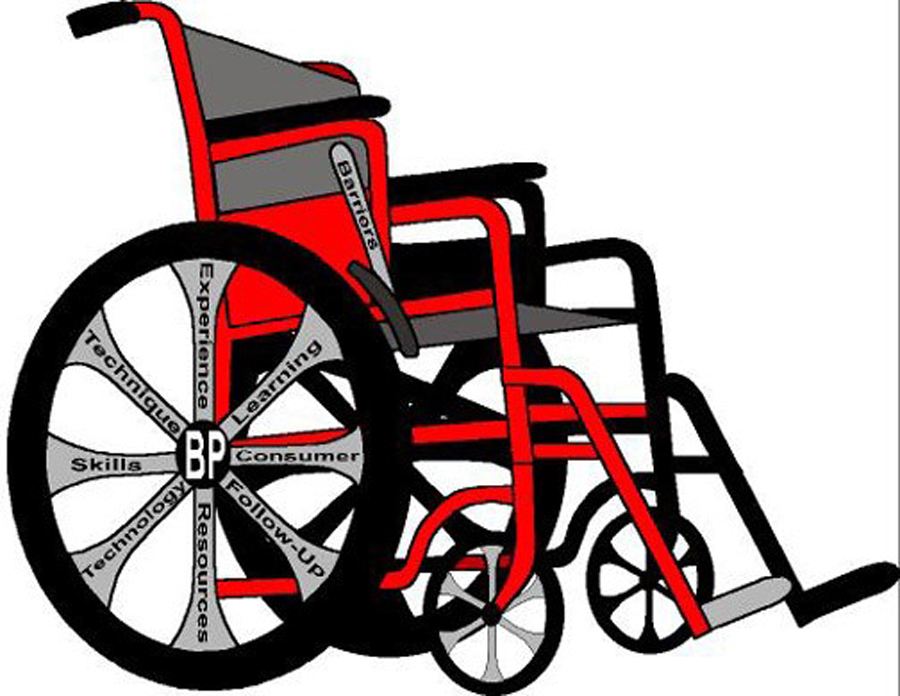
The metaphor of the wheel depicts best practice as defined by the results of this research (Click for larger view)
Best practices in the area of seating and mobility can best be depicted by the metaphor of the wheel (Fig. 1). In this metaphor, the hub represents the concept of best practices. Around that hub are all the concepts identified by the panel as necessities. These are represented by spokes. The spokes include: (a) experience, (b) hands on techniques, (c) skills, (d) technology, (e) resources, (f) self-directed learning, (g) follow-up, and (h) consumer relationships. If a spoke is missing or broken, the wheel does not run smoothly. Also included are the barriers, which can best be represented by the brake. On a wheelchair, just as a brake can slow or stop the wheel, so barriers can be a hindrance on the road to best practice. However, as noted by this panel of expert practitioners, these barriers can and should be overcome.
Experience
Experts tend to know more about contexts, and their knowledge tends to be more organized and efficient than novices. Experts are individuals that have learned through experience. They are more likely than novices to utilize relevant information, they are less likely to be influenced by irrelevant cues than novices, and they are less likely to be overconfident (5). They do not create solutions from scratch for every problem situation. Instead, they make use of previously stored information in such a way that facilitates coping with current problems (6). They have a thorough understanding of how to organize, represent, and interpret learned concepts in their environments, which affects their ability to remember, reason, and solve problems (7). Their experience takes them to a high level of concept formation.
Hands on Techniques
This group of highly skilled therapists recognized and identified that their skill acquisition and implementation has progressed to a higher level. It is the ability to find the groove. Therapists may make conscious decisions that should be based on research and theories. However therapists are also dependent on tacit recognitions, judgments, and skillful performances. Reflection-in-action takes knowing-in-action to a higher level.
Skills
A number of skills were identified in Round 1 that are necessities for thorough implementation of a seating and mobility evaluation. Specifically, the skills included (a) the ability to perform a thorough mat assessment, (b) the ability to simulate the desired position through utilization of a seating simulator or trial equipment, (c) the ability to utilize and interpret a pressure mapping system, (d) the ability to apply bio-mechanical anatomical knowledge appropriately to the situation, which includes a thorough movement assessment, (e) the ability to complete a thorough environmental assessment, and (f) the ability to perform a complete and thorough interview.
Technology
An understanding of technology available and strengths and weaknesses of the technology allows the therapist to make sound realistic decisions about its use and application. Without this knowledge and understanding, unrealistic goals might be established both by the evaluator and by the consumer. This can potentially lead to failure of the seating and mobility system to meet the needs of the consumer, and can lead to frustrations and even harm.
Best practice involves an understanding of basics combined with up-to-date knowledge of new knowledge and the ability to use the two together. This includes an understanding and application of “old technology” and “new technology”. Not only is understanding of both technologies important, but the ability to analyze and combine the two also separates novice from expert.
Resources
The only man who is educated is the man who has learned how to learn and how to adapt and change (8). This involves the learning how to learn concept. A key component to this concept is the ability to know how to plan, evaluate, and select resources (9). This group of expert practitioners recognized the necessity of this skill and has gained the skill. They have learned which resources to use and not to use and to use those resources well.
Self-Directed Learning
In the dynamic field of assistive technology, and more specifically seating and mobility, much of the information quickly evolves and changes. Therapists must be active in their own search for additional knowledge and skills. Although experience was identified by 100% of the participants as the method with which they have gained the majority of their skills and knowledge, these skills and knowledge have not been gained through experience alone.
Follow-Up
Once an evaluation is completed, a plan developed, and the plan implemented, it must be determined whether the recommendations and the plan worked. Follow-up is identified as the best method for this confirmation. Follow-up was identified and defined as both formal and informal in nature. Both forms of follow-up are extremely useful. Ideally, both forms of follow-up should be utilized.
Consumer Relations
Consumers know best their needs, goals, and desires. Expert practitioners who participated in this research project are all very aware of the important part that the consumer plays in the seating and mobility evaluation process. As put by one participant, “They know more about themselves and their needs than I will ever learn through any evaluation process.” They recognize that they must not be just skilled therapists, but also that they must be good listeners. Identification and recognition of the consumer brings the model of best practices full circle.
Barriers
The clinician recognizes that barriers can and do exist which may interfere with a thorough seating and mobility evaluation. However, constant efforts should be made to overcome these barriers. The first step in overcoming barriers is identification of the barriers. Barriers that currently exist in the area of seating and mobility included time restraints, limited funding, unavailability of equipment for trials, and limited access for the completion of an environmental assessment. Experience has helped these clinicians recognize that barriers do exist that can be overcome. Creativity and the ability to think outside of the box are skills which these therapists have developed and utilized to overcome these barriers.
CONCLUSIONS
Best practices are the foundation on which standards of practice are built. As a result of this research project, best practices are depicted by the metaphor of the wheel (Fig. 1). In this metaphor, the hub represents the concept of best practices. Around that hub are all the concepts that were identified by the panel as necessities for the implementation of best practices in the areas of seating and mobility. These are represented by spokes. The spokes include (a) experience, (b) hands on techniques, (c) skills, (d) technology, (e) resources, (f) self directed learning, (g) follow-up, and (h) consumer relationships. If a spoke is missing or broken, the wheel does not run smoothly. Also included are the barriers, which can best be represented by the brake. On a wheelchair, just as a brake can slow or stop the wheel, so barriers can be a hindrance on the road to best practice. However, these barriers can and should be overcome.
REFERENCES
- Dunn, W. (2000). Best practice occupational therapy. Thorofare, NJ: SLACK Incorporated.
- Linstone, H.A., & Turoff, M. (1975). The Delphi Method: techniques and applications. Reading, MA: Addison-Wesley Publishing Company.
- Hasson, F. Keeney, S. McKenna, H. (2000). Research guidelines for the Delphi survey technique. Journal of Advanced Nursing, 32(4): 1008-1015.
- Jenson, G. M., Gwyer, J., Shepard, K. F., & Hack, L. M. (2000). Expert practice in physical therapy. Physical Therapy, 80, 28-43.
- Byrnes, J. P. (1998). The nature and development of decision making. Mahwah, New Jersey: Lawrence Erlbaum Associates, Publishers.
- Sternberg, R. J. (1990). Metaphors of mind: Conception of the nature of intelligence. New York: Cambridge University Press.
- Shelton, F. (2003). Adult learning: Cognitive foundations for learning a complex computer based task. Unpublished doctoral dissertation. Oklahoma State University, Stillwater.
- Rogers, C. (1969). Freedom to learn. Columbus, OH: Merrill Publishing.
- Smith, R. M. (1982). Learning how to learn applied theory for adults. Chicago: Follett Publishing Company.
- Rotondi, A., & Gustafson, D. 1996. Theoretical, methodological and practical issues arising out of the Delphi method. In Gazing into the Oracle: The Delphi method and its application to social policy and public health Edited by: Adler, M., & Ziglio, E. Bristol, PA: Jessica Kingsley Publishers, Ltd; 34-55.
Mary Isaacson
OU-Tulsa
4502 East 41st Street
Rm. 2J34
Tulsa, OK 74135
918-660-3272
Mary-isaacson@ouhsc.edu